Guide
Postpartum Anxiety vs Depression: Key Differences
By Dr. Naomi Walsh, MD (OB/GYN) · Updated 2026-03-10
Postpartum anxiety and postpartum depression are two distinct conditions that often overlap — and both are far more common than most people realise. Anxiety is actually more prevalent than depression after birth, yet it's far less discussed. Understanding the difference between the two is the first step to getting the right help for what you're actually experiencing.
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. If you are experiencing postpartum mental health symptoms, please consult a qualified healthcare provider. If you are in crisis, contact the Postpartum Support International helpline at 1-800-944-4773 or your local emergency services.
Affiliate Disclosure: This post contains affiliate links. We may earn a commission at no extra cost to you.
By Dr. Naomi Walsh, MD (OB/GYN) — Last updated March 2026
Table of Contents
- What Is Postpartum Anxiety?
- What Is Postpartum Depression?
- Symptom Comparison Table
- Diagnostic Criteria
- Treatment Options
- When to Seek Help Immediately
- Postpartum Recovery Products
- Frequently Asked Questions
- Sources & Methodology
What Is Postpartum Anxiety?

Postpartum anxiety (PPA) affects approximately 10–15% of new mothers — making it roughly as common as postpartum depression and in some studies more common. Yet it receives significantly less attention in public health messaging, leaving many women undiagnosed and untreated.
PPA is not simply "new parent worrying." All new parents worry. Postpartum anxiety is a clinical condition characterised by anxiety that is persistent, excessive, and disproportionate — anxiety that interferes with your ability to function, sleep, or care for yourself and your baby.
Core Symptoms of Postpartum Anxiety
Psychological symptoms:
- Constant, racing worry about the baby's health, safety, or development
- Inability to stop worst-case-scenario thinking (catastrophising)
- Feeling of impending doom or danger
- Intrusive, unwanted thoughts (often distressing "what if I drop the baby" scenarios)
- Hypervigilance — watching the baby's breathing obsessively, needing constant reassurance
- Difficulty making decisions or concentrating
- Irritability and anger that feels disproportionate
Physical symptoms:
- Muscle tension, jaw clenching, shoulder tightness
- Racing heart, palpitations
- Shortness of breath
- Nausea or stomach upset
- Dizziness or lightheadedness
- Difficulty sleeping even when the baby is asleep (can't "switch off")
- Hot flashes or sweating
Postpartum OCD: A Related Condition
Postpartum OCD (obsessive-compulsive disorder) is related to PPA but distinct. It involves intrusive, ego-dystonic thoughts — thoughts that horrify you, that you don't want to have — often about harm coming to the baby. Importantly, postpartum OCD thoughts are not a sign that you want to harm your baby. The very distress these thoughts cause indicates the opposite. This condition is highly treatable but requires specific therapy approaches (ERP — exposure and response prevention).
What Is Postpartum Depression?

Postpartum depression (PPD) is a major depressive episode occurring in the context of childbirth. It affects approximately 10–15% of new mothers (some studies put the figure higher, at 1 in 5) and requires clinical diagnosis and treatment.
PPD is not:
- "Baby blues" — the normal emotional adjustment that affects 50–80% of new mothers in the first 2 weeks and typically resolves on its own
- Weakness or failure
- A sign you are a bad mother
- Something that will resolve without support
PPD can begin during pregnancy (perinatal depression), in the first weeks after birth, or gradually emerge over the first year postpartum. It is most common in the first 3 months.
Core Symptoms of Postpartum Depression
Emotional symptoms:
- Persistent sadness, emptiness, or hopelessness that doesn't lift
- Loss of interest in activities you previously enjoyed
- Feeling disconnected from or indifferent to your baby (not feeling the love you "should")
- Feeling like a failure as a mother
- Excessive guilt or shame
- Feeling trapped or overwhelmed without a specific worry
Cognitive symptoms:
- Difficulty concentrating or making decisions
- Negative thought patterns about yourself, the future
- Thoughts of not wanting to be here (in severe cases, suicidal thoughts — seek help immediately)
Physical symptoms:
- Persistent fatigue far beyond normal new parent tiredness
- Appetite changes (eating too much or too little)
- Sleep disruption beyond infant-caused waking (can't sleep even when able)
- Physical heaviness, moving and speaking slowly
- Unexplained physical complaints (headaches, digestive issues)
Postpartum Psychosis: A Rare Emergency
Postpartum psychosis is distinct from both PPD and PPA. It is rare (1–2 per 1,000 births) but a medical emergency. Symptoms include hallucinations, delusions, severe confusion, paranoia, and erratic behaviour, typically emerging within the first 2 weeks postpartum. This requires immediate hospitalisation and treatment.
Symptom Comparison Table

| Feature | Postpartum Anxiety (PPA) | Postpartum Depression (PPD) |
|---|---|---|
| Primary emotion | Fear, worry, dread | Sadness, emptiness, numbness |
| Mental state | Racing, overactive thoughts | Slowed, foggy, empty |
| Baby connection | Overattached, hypervigilant about baby | May feel disconnected or indifferent |
| Sleep disruption | Can't sleep even when possible; mind won't stop | Hypersomnia OR insomnia; general fatigue |
| Appetite | Often decreased (stomach upset) | Increased or decreased; often disinterested in food |
| Physical symptoms | Racing heart, tension, shortness of breath | Fatigue, physical heaviness, psychomotor slowing |
| Interest in activities | Often wants engagement but feels too anxious to relax | Loss of interest in things previously enjoyed |
| Good moments | Can have good moments when distracted | Persistent low mood, even good events feel flat |
| Prevalence | ~15% of new mothers | ~10–15% (some studies up to 20%) |
| Can occur together? | Yes — up to 50% of PPD cases also involve significant anxiety. Both can coexist. | |
Diagnostic Criteria
Screening Tools
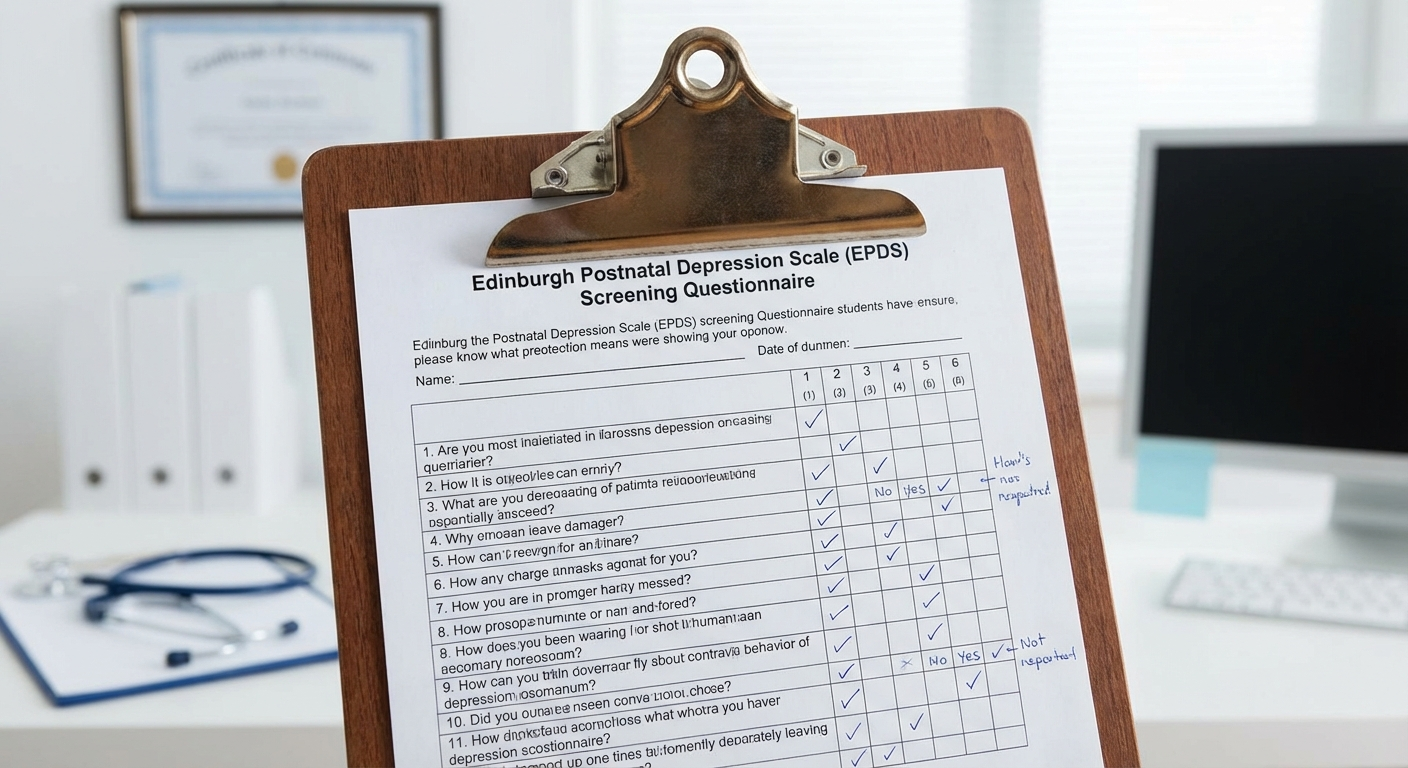
The Edinburgh Postnatal Depression Scale (EPDS) is the gold standard screening tool for postpartum mental health. It's a 10-question self-report questionnaire designed to identify both depression and anxiety symptoms in the postpartum period. Most healthcare providers should administer it at the 6-week postpartum appointment — if yours doesn't, ask for it.
EPDS scoring:
- 0–8: Likely not experiencing PPD/PPA
- 9–11: May be developing symptoms — monitoring recommended
- 12+: Likely experiencing PPD or PPA — clinical assessment warranted
- Any score on question 10 (thoughts of self-harm): immediate clinical assessment required
For anxiety specifically, the Generalised Anxiety Disorder scale (GAD-7) is commonly used alongside the EPDS.
When Does PPD/PPA Require Clinical Diagnosis?
A clinical diagnosis of PPD or PPA requires:
- Symptoms present for more than 2 weeks (rules out normal baby blues)
- Symptoms causing clinically significant impairment in functioning (parenting, relationships, self-care)
- Symptoms not better explained by another medical condition (e.g. thyroid dysfunction, iron deficiency — both common postpartum and both mimick depression/anxiety)
Before any psychiatric diagnosis, a thyroid function test (TSH, T3, T4) and full blood count should be run to rule out physical causes.
Treatment Options

Both PPD and PPA are highly treatable conditions. Most women recover fully with appropriate support. Treatment options range from self-care strategies for mild symptoms to medication for moderate-to-severe cases.
Psychotherapy
Cognitive Behavioural Therapy (CBT) is first-line treatment for both PPD and PPA. CBT addresses the thought patterns that maintain both conditions:
- For PPA: challenges catastrophic thinking and "what if" spirals
- For PPD: addresses negative self-beliefs and hopelessness
Interpersonal Therapy (IPT) is specifically validated for postpartum depression and focuses on the relationship changes that come with new parenthood.
Both therapies have strong evidence bases in the perinatal period and are safe for breastfeeding mothers.
Medication
For moderate-to-severe PPD and PPA, antidepressants may be recommended. SSRIs (selective serotonin reuptake inhibitors) are first-line:
- Sertraline (Zoloft) — most evidence for safety in breastfeeding
- Paroxetine — also well-studied in breastfeeding
- Fluoxetine — used but passes into breast milk at higher levels
The decision to use medication during breastfeeding should be made with a psychiatrist or prescribing physician who specialises in perinatal mental health. The risks of untreated severe PPD/PPA to both mother and baby are generally considered greater than the risks of appropriately managed medication.
Lifestyle and Self-Care
While not a substitute for clinical treatment in moderate-to-severe cases, these are meaningful adjuncts:
- Sleep prioritisation: Postpartum sleep deprivation significantly worsens both anxiety and depression — arrange support so you can sleep in 4+ hour uninterrupted blocks when possible.
- Physical activity: Even gentle walking has demonstrated effects on mood and anxiety in the postpartum period.
- Social support: Isolation is a major risk factor. Joining a postpartum support group (online or in-person) provides peer understanding that family members often can't.
- Nutritional support: Omega-3 fatty acids, iron (if deficient), and vitamin D have supporting evidence in perinatal mental health.
Peer Support
Postpartum Support International (PSI) operates a free helpline (1-800-944-4773) and an online support community. It offers a provider directory to find perinatal mental health specialists in your area. This is a legitimate and valuable first resource.
When to Seek Help Immediately
For a complete overview of postpartum physical recovery, see our guide on the postpartum recovery guide — which covers the full spectrum of healing in the months after birth.
Contact your healthcare provider or emergency services immediately if you experience:
- Thoughts of harming yourself or your baby (even fleeting — this needs evaluation)
- Inability to care for your baby due to mental health symptoms
- Feeling detached from reality, hearing voices, or experiencing delusions (possible postpartum psychosis — medical emergency)
- Inability to eat or sleep at all for multiple days
- Total inability to function in daily life
Also see our guide on postpartum recovery week by week for a broader understanding of the physical and emotional timeline after birth.
And for physical recovery support, see: best postpartum support belts — rated for both comfort and practical postpartum use.
Postpartum Recovery Products
Postpartum Mental Health Journal — Best Mood Tracker
Best for: Tracking symptoms, preparing for appointments, daily check-ins
Feature: Guided prompts, mood tracking, self-care planning
Benefit: Externalising anxiety thoughts reduces their power
Price: $
Check on Amazon →
LectroFan White Noise Machine — Best Sleep Aid
Best for: Improving postpartum sleep quality during available windows
Feature: 20 unique sounds, consistent white noise, compact
Benefit: Better sleep quality reduces anxiety and depression risk
Price: $$
Check on Amazon →
Nordic Naturals Postnatal Omega-3 — Best Supplement
Best for: Supporting mood in postpartum recovery
Feature: 1120mg DHA + EPA, safe for breastfeeding, third-party tested
Evidence: EPA shown to reduce depressive symptoms in perinatal studies
Price: $$
Check on Amazon →
"Good Moms Have Scary Thoughts" by Karen Kleiman — Best Book
Best for: Understanding intrusive thoughts, postpartum OCD, anxiety
Feature: Evidence-based, non-judgmental, illustrated approach
Benefit: Normalises common postpartum anxious thoughts
Price: $
Check on Amazon →
Belly Bandit Viscose Bamboo Wrap — Best Physical Recovery
Best for: Abdominal support, easing physical discomfort postpartum
Feature: Medical-grade compression, adjustable, breathable
Benefit: Physical comfort supports emotional recovery
Price: $$
Check on Amazon →
Verilux HappyLight Therapy Lamp — Best Light Therapy
Best for: Postpartum depression, especially in winter months
Feature: 10,000 lux, UV-free, 15–20 min daily use
Evidence: Bright light therapy has demonstrated benefit in perinatal depression
Price: $$
Check on Amazon →Frequently Asked Questions
Can you have postpartum anxiety and depression at the same time? Yes — and it's common. Studies suggest that up to 50% of women with postpartum depression also experience significant anxiety. The two conditions share risk factors, often develop together, and respond to similar treatments (CBT, SSRIs). Being diagnosed with one doesn't rule out the other.
How long does postpartum anxiety typically last? Without treatment, PPA can persist for months or years. With appropriate treatment (therapy, medication if needed), most women see significant improvement within 6–12 weeks. Early intervention leads to faster and more complete recovery. Don't wait to see if it improves on its own.
Is postpartum anxiety normal? Some degree of heightened concern for your newborn is normal and adaptive — it keeps babies safe. What crosses into clinical postpartum anxiety is when the worry is excessive, uncontrollable, disproportionate, and interferes with functioning or sleep. If you're questioning whether your anxiety is "normal," that uncertainty is itself a reason to discuss it with your provider.
Can fathers and non-birthing parents get postpartum depression or anxiety? Yes. Research shows that approximately 10% of fathers experience paternal postpartum depression, typically peaking at 3–6 months after birth. Non-birthing parents of any gender can also develop postpartum anxiety. The same screening tools and treatments apply.
Does postpartum anxiety affect my ability to bond with my baby? Postpartum anxiety can paradoxically make bonding harder — hypervigilance and physical tension make it difficult to be relaxed and present with your baby. Postpartum depression more commonly presents with bonding difficulties. Both conditions respond well to treatment, and bonding typically improves significantly as symptoms are addressed.
Are there natural or non-medication treatments for postpartum anxiety? For mild PPA, therapy alone (especially CBT) is often sufficient. Exercise, sleep prioritisation, omega-3 supplementation, and peer support all have supporting evidence. For moderate-to-severe PPA, medication is often necessary for adequate recovery and should not be avoided out of fear — untreated severe anxiety has real consequences for both mother and baby.
Sources and Methodology
Written by Dr. Naomi Walsh, MD, OB/GYN, with specialist review in perinatal mental health.
Medical disclaimer: This article provides general information only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider with questions about your mental health.
- O'Hara MW, Wisner KL. "Perinatal mental illness: definition, description and aetiology." Best Practice & Research Clinical Obstetrics & Gynaecology, 2014. DOI: 10.1016/j.bpobgyn.2013.09.002
- Postpartum Support International (PSI) — Prevalence statistics, treatment guidelines, and peer support resources. postpartum.net
- Cox JL, et al. "Detection of postnatal depression: development of the 10-item Edinburgh Postnatal Depression Scale." British Journal of Psychiatry, 1987. DOI: 10.1192/bjp.150.6.782
- Dennis CL, Dowswell T. "Psychosocial and psychological interventions for preventing postpartum depression." Cochrane Database of Systematic Reviews, 2013.
- American Psychiatric Association. DSM-5: Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (Peripartum onset specifier, Major Depressive Episode).
Crisis Resources:
- Postpartum Support International Helpline: 1-800-944-4773
- National Suicide Prevention Lifeline: 988
- Crisis Text Line: Text HOME to 741741
Dr. Naomi Walsh, MD, is an obstetrician/gynaecologist with subspeciality training in perinatal mental health. She has cared for women through pregnancy and postpartum recovery for 18 years and is an advocate for routine perinatal mental health screening.