Guide
Fourth Trimester: What Nobody Tells You
By Dr. Nina Chen, OB-GYN & Postpartum Specialist · Updated 2026-03-10
The fourth trimester — the first 12 weeks after birth — is the most physically and emotionally demanding period most women will ever face. Your body is healing from a major medical event, your hormones are in freefall, and you are learning to keep a tiny human alive on almost no sleep. This evidence-based guide covers what actually happens during the fourth trimester, what is normal versus what needs medical attention, and which recovery products are worth your money.
By Dr. Nina Chen, OB-GYN & Postpartum Specialist | Last updated: March 2026
Table of Contents
- What Is the Fourth Trimester?
- Physical Recovery: What Is Really Happening to Your Body
- Emotional and Mental Health in the Fourth Trimester
- Your Newborn in the Fourth Trimester
- Building a Support System That Actually Works
- Self-Care Strategies for the Fourth Trimester
- Fourth Trimester Recovery Essentials
- Week-by-Week Fourth Trimester Timeline
- When to Call Your Doctor
- FAQ: Fourth Trimester
- Sources
What Is the Fourth Trimester?
The term "fourth trimester" was popularised by paediatrician Dr. Harvey Karp, but the concept has deep roots in maternal health. It refers to the first 12 weeks after birth — a period the American College of Obstetricians and Gynecologists (ACOG) now recognises as a critical window for maternal health and wellbeing.
Here is what nobody tells you: this period is not just about recovery. It is a complete physiological and psychological transformation. Your body is simultaneously healing from a major medical event, establishing (or choosing not to establish) a milk supply, adjusting to radical hormonal shifts, and rewiring your brain — literally. Neuroimaging studies published in Nature Neuroscience show that the maternal brain undergoes structural changes that persist for at least two years after birth.
Yet despite the enormity of this transition, modern healthcare systems typically offer a single six-week postpartum check-up and then send new mothers on their way. That gap between what women experience and what the system supports is exactly why the fourth trimester matters — and why understanding it can make the difference between struggling in silence and recovering with confidence.
If you are currently in the early weeks, our postpartum recovery week-by-week guide walks through exactly what to expect at each stage. This guide takes a wider lens, covering the physical, emotional, relational, and practical dimensions of the entire fourth trimester.
Physical Recovery: What Is Really Happening to Your Body
The physical recovery that takes place in the fourth trimester is staggering in scope. Here is a systems-level breakdown of what your body is doing.
Uterine Involution
Immediately after delivery, your uterus weighs roughly 1 kilogram. Over the next six weeks it contracts back to its pre-pregnancy weight of around 60 grams — a reduction of more than 90%. This process, called involution, produces afterpains: cramping contractions that can range from mildly uncomfortable to genuinely painful, especially in women who have had previous births. Breastfeeding intensifies these cramps because oxytocin — the same hormone that triggers milk letdown — also stimulates uterine contractions.
Lochia: The Bleeding Nobody Prepares You For
Postpartum bleeding (lochia) occurs regardless of whether you had a vaginal or caesarean delivery. It is not a period. It is your uterus shedding the thick lining it built to support your pregnancy.
- Days 1–3: Heavy, bright red, may include small clots
- Days 4–10: Gradually lightens to pinkish-brown
- Weeks 2–4: Becomes yellowish-white (lochia alba)
- Weeks 4–6: Tapers off and stops
Soaking through more than one pad per hour, passing clots larger than a golf ball, or a sudden return of bright red bleeding after it has lightened are not normal and require immediate medical attention.
Perineal and Caesarean Recovery
Around 85% of women who deliver vaginally experience some degree of perineal tearing. First- and second-degree tears typically heal within two to four weeks. Third- and fourth-degree tears — which extend into the anal sphincter — may take considerably longer and can cause lasting pelvic floor issues if not managed with physiotherapy.
Caesarean recovery involves healing from major abdominal surgery. The external incision is only part of the picture; internally, seven distinct layers of tissue were cut and sutured. Most women begin to feel significantly better by four to six weeks, but full tissue healing takes three to six months. Numbness, tingling, and itching around the scar are normal for months and sometimes years.
Hormonal Freefall
Within 24 hours of delivering the placenta, oestrogen and progesterone levels plummet by more than 90%. This is the most dramatic hormonal shift the human body experiences in such a short timeframe. The consequences ripple through every system:
- Mood regulation: The sharp drop in oestrogen affects serotonin production, contributing to mood swings and vulnerability to depression
- Thermoregulation: Night sweats are common as your body recalibrates
- Hair: The lush pregnancy hair you enjoyed begins to shed around months 2–4 (see our postpartum hair loss guide)
- Joints and ligaments: Relaxin remains elevated for weeks to months, keeping joints looser and more injury-prone
- Thyroid: Up to 10% of postpartum women develop postpartum thyroiditis, which can mimic depression or anxiety
Pelvic Floor: The Foundation You Cannot See
Pregnancy and vaginal delivery place enormous strain on the pelvic floor — the hammock of muscles that supports your bladder, uterus, and rectum. Studies show that up to 35% of first-time mothers experience urinary incontinence in the postpartum period, and approximately 50% have some degree of pelvic organ prolapse (most cases are mild).
Pelvic floor recovery is not optional. It is foundational. Gentle pelvic floor exercises (Kegels) can usually begin within the first few days after a vaginal birth, once any acute pain has subsided. Our detailed pelvic floor exercise guide provides a progressive programme from week one through month six.
Abdominal Separation (Diastasis Recti)
Up to 60% of postpartum women have some degree of diastasis recti — a separation of the rectus abdominis muscles along the midline. This is not just cosmetic; it can cause lower back pain, pelvic instability, and a persistent "pooch" that no amount of crunches will fix (in fact, crunches can make it worse). Our complete diastasis recti recovery exercise guide covers self-testing, safe movements, and when to seek physiotherapy.
Emotional and Mental Health in the Fourth Trimester
If the physical recovery is the part nobody prepares you for, the emotional landscape is the part nobody talks about honestly. The fourth trimester can be joyful, terrifying, boring, overwhelming, and heartbreaking — sometimes all in the same hour.
Baby Blues vs. Postpartum Depression vs. Postpartum Anxiety
Baby blues affect up to 80% of new mothers. They typically begin around day 3–5 (when milk comes in and the hormonal crash peaks) and resolve within two weeks. Symptoms include tearfulness, irritability, overwhelm, and mood swings. Baby blues are normal and do not require treatment.
Postpartum depression (PPD) is a clinical condition that affects approximately 1 in 7 new mothers. It differs from baby blues in severity, duration, and impact on functioning. Symptoms include persistent sadness, loss of interest in things you used to enjoy, difficulty bonding with your baby, changes in appetite or sleep beyond what baby-related disruption causes, feelings of worthlessness or guilt, and in severe cases, thoughts of self-harm. PPD can begin any time in the first year but most commonly appears between weeks 4 and 12. For a deeper look at symptoms and treatment, see our postpartum depression guide.
Postpartum anxiety (PPA) is increasingly recognised as equally common but is diagnosed less often because anxious new mothers are frequently dismissed with "all new mums worry." PPA involves persistent, intrusive worry that interferes with daily life — racing thoughts, an inability to relax even when the baby is safe, physical symptoms like heart palpitations and nausea, and sometimes panic attacks. Our guide on postpartum anxiety vs. depression explains how to tell the difference and where to find help.
The Identity Shift Nobody Warns You About
Becoming a mother (or becoming a mother again) fundamentally reorganises your sense of self. Psychologists call this "matrescence" — a developmental transition as significant as adolescence. You may grieve the loss of your pre-baby identity, your freedom, your relationship as it was, or your career momentum. These feelings are not a sign that you are ungrateful or failing. They are a sign that you are human and undergoing a seismic life change.
Bonding Is Not Always Instant
Perhaps the most harmful myth in modern parenting culture is that bonding happens immediately. For many women it does. For many others it does not. Exhaustion, birth trauma, pain, hormonal chaos, and the sheer shock of new parenthood can delay the rush of attachment. Research published in the Archives of Women's Mental Health shows that consistent responsive caregiving — not a single magical moment — is what builds secure attachment over time. If you do not feel an immediate overwhelming love for your baby, you are not broken. You are normal.
Intrusive Thoughts
Up to 90% of new parents experience intrusive thoughts — sudden, unwanted mental images of harm coming to their baby. These thoughts are distressing precisely because they are the opposite of what you want. They are a feature of a hypervigilant postpartum brain, not a sign that you are dangerous. However, if intrusive thoughts become persistent, are accompanied by compulsive behaviours (such as repeatedly checking whether the baby is breathing), or cause you to avoid your baby, speak with your provider. These may indicate postpartum OCD, which responds well to treatment.
Your Newborn in the Fourth Trimester
The fourth trimester is a two-way experience. While you are recovering, your baby is making the most dramatic environmental transition of their life — from the dark, warm, constantly held, never-hungry world of the womb to the bright, cold, sometimes-alone, sometimes-hungry world outside.
Why Your Baby Wants to Be Held Constantly
Human babies are born neurologically immature compared to other mammals. A newborn horse can walk within hours; a human baby cannot hold up its own head. Dr. Karp's fourth trimester theory suggests that human babies are essentially born three months early (relative to neurological development) because of the constraints of the human pelvis.
This means your baby is not "manipulating" you when they cry the moment you put them down. They are responding to a biological imperative: in evolutionary terms, a baby alone is a baby in danger. Holding, rocking, swaddling, and shushing replicate womb conditions and activate calming reflexes.
The Crying Peak
Infant crying typically peaks between weeks 6 and 8, when many babies cry for 2–3 hours per day (sometimes more). This is often called the "period of PURPLE crying." It is developmental, not a sign that something is wrong or that you are doing something wrong. It does, however, tend to coincide with peak maternal exhaustion and the expiry of any help from visitors — a perfect storm that contributes to the fourth trimester's reputation as the hardest phase of early parenthood.
Feeding in the Fourth Trimester
Whether you breastfeed, formula feed, or combination feed, the fourth trimester is feeding-intensive. Newborns feed 8–12 times per day, and breastfed babies may cluster feed for hours at a time, particularly in the evenings. This is normal — it is not a sign of low supply.
Common fourth trimester feeding challenges include:
- Painful latch or nipple damage (a lactation consultant can help)
- Engorgement when milk comes in (days 2–5)
- Growth spurts at around 2 weeks, 3 weeks, and 6 weeks
- Reflux and colic symptoms
- The pressure and guilt surrounding feeding choices
As your baby grows and begins to approach the end of the fourth trimester, you may start thinking about the next nutritional phase. For guidance on introducing first foods, starting solids after the fourth trimester is an excellent evidence-based resource.
Sleep (or the Lack of It)
Newborns do not have a circadian rhythm. They sleep in short bursts of 2–4 hours around the clock, with no concept of day or night. This means you will experience cumulative sleep deprivation that, by week 6, can rival the cognitive impairment of being legally intoxicated. This is not hyperbole — studies show that postpartum sleep deprivation impairs reaction time, decision-making, and emotional regulation to a degree comparable to a blood alcohol level of 0.05–0.10%.
Safe sleep practices (baby on their back, on a firm flat surface, in the same room but not the same bed, with no loose bedding) are non-negotiable. But beyond safety, "sleep when the baby sleeps" is well-meaning advice that ignores the reality that some babies only sleep while being held and that daytime sleep is lighter and less restorative than nighttime sleep.
Building a Support System That Actually Works
The single greatest predictor of positive postpartum outcomes is not wealth, fitness, or even physical health — it is the quality and availability of social support. Yet many new mothers find themselves more isolated than at any other point in their lives.
The Village Myth
"It takes a village" is true, but the village does not exist for most modern families. Extended families live far away, parental leave is inadequate (or nonexistent), and the culture of self-sufficiency makes asking for help feel like failure. Building a support system in the fourth trimester requires deliberate effort and a willingness to be vulnerable.
Practical Support Strategies
Before birth:
- Accept every offer of help — and be specific about what you need. "Could you drop off a meal on Tuesday?" is easier for people to act on than "Let us know if you need anything."
- Stock your freezer with meals, or set up a meal train through apps like MealTrain or Signup Genius
- Identify one or two people who can be "on call" for emotional support during difficult moments
After birth:
- Limit visitors in the first two weeks. Well-meaning guests often create more work than relief.
- Join a postnatal group — either in person or online. Connection with other women in the same stage of motherhood is protective against depression and isolation.
- Consider hiring a postpartum doula if your budget allows. Research published in Birth journal shows that postpartum doula support is associated with reduced depression, improved breastfeeding outcomes, and greater parenting confidence.
Partners in the Fourth Trimester
Partners undergo their own fourth trimester. Studies show that testosterone drops and oxytocin rises in new fathers during the postpartum period. Approximately 10% of new fathers experience paternal postnatal depression — a figure that rises to 50% when the birthing partner has PPD. The fourth trimester often exposes cracks in relationships because both parties are depleted, scared, and navigating a version of their partner they have not met before.
What helps: explicit communication about needs, fair (not necessarily equal) division of night feeds and household tasks, maintaining physical affection even when sex is off the table (it is recommended to wait until at least 6 weeks and full healing), and recognising that this phase is temporary.
Self-Care Strategies for the Fourth Trimester
"Self-care" in the fourth trimester is not bath bombs and face masks. It is the bare minimum of keeping yourself alive and functional so that you can keep your baby alive and functional. Here is what actually helps.
Sleep Preservation
Sleep is the single most impactful thing you can protect. Strategies include:
- Splitting the night with your partner (e.g., you sleep 8pm–1am while they handle feeds, then switch)
- Having a partner give one bottle of expressed milk or formula so you get a longer stretch
- Sleeping in a dark, cool room with earplugs during your "off" shift (the on-duty parent uses a monitor)
- Napping when possible — even 20 minutes reduces cortisol and improves mood
Nutrition
Your body needs serious fuel to heal. If you are breastfeeding, you need approximately 500 extra calories per day. Focus on:
- Protein at every meal (eggs, Greek yoghurt, nuts, lean meats) for tissue repair
- Iron-rich foods (red meat, lentils, spinach) to replenish stores lost during birth
- Omega-3 fatty acids (oily fish, walnuts, flaxseed) for brain health and mood regulation
- Hydration — dehydration worsens fatigue and can reduce milk supply
Movement
Gentle movement supports recovery. In the first two weeks, this means short walks (even 10 minutes) and pelvic floor exercises. By weeks 4–6, you may be ready for postnatal yoga or Pilates. Avoid high-impact exercise, heavy lifting, and abdominal crunches until you have been assessed for diastasis recti and given clearance by your provider.
Mental Health Maintenance
- Lower the bar. Dramatically. A successful day in the fourth trimester is one where you and the baby are fed, clean-ish, and alive.
- Get outside daily. Sunlight exposure helps regulate circadian rhythm (yours and the baby's) and supports vitamin D production.
- Stay connected. Send a voice note to a friend. Join a group chat with other new parents. Isolation is the enemy.
- Monitor your mood using a validated screening tool like the Edinburgh Postnatal Depression Scale (EPDS). If your score is 10 or above, or if you have any thoughts of self-harm, contact your healthcare provider immediately.
Fourth Trimester Recovery Essentials
After reviewing dozens of postpartum products and consulting with pelvic floor physiotherapists, these are the items that make a genuine difference in fourth trimester recovery. Each has been selected based on clinical utility, patient feedback, and value.
1. Frida Mom Postpartum Recovery Essentials Kit
Best Overall Fourth Trimester Kit
Everything you need in one box: perineal healing foam, disposable underwear, ice maxi pads, and a peri bottle. Designed by mothers for mothers, this kit addresses the mess and discomfort that nobody warns you about.
- Perineal foam with witch hazel for soothing relief
- Disposable underwear that actually stays up
- Instant ice maxi pads for swelling reduction
- Upside-down peri bottle for easy, one-handed use
Why we recommend it: Eliminates the guesswork of buying individual products. Hospital-grade quality without the hospital markup.
2. Belly Bandit Original Belly Wrap
Best Postpartum Belly Support
Medical-grade compression that supports your abdominal wall and lower back during the critical first weeks of recovery. Helps with posture, reduces swelling, and provides gentle proprioceptive feedback that reminds you to engage your core.
- Adjustable compression with Velcro closures
- Latex-free, breathable fabric
- Can be worn over or under clothing
- Sizing from XS to XXL
Why we recommend it: Backed by research showing compression garments reduce pain and improve mobility after both vaginal and caesarean births. See our best postpartum support belts guide for full comparisons.
3. Haakaa Silicone Breast Pump
Best Passive Milk Collection
This simple silicone pump attaches to the non-nursing breast via suction and collects letdown milk that would otherwise be absorbed by a nursing pad. Many mothers collect 30–120ml per feed without any effort.
- One piece — no cords, batteries, or parts to wash
- BPA-free, food-grade silicone
- Suction base prevents spills
- Pairs perfectly with the included flower stopper
Why we recommend it: Building a small freezer stash without adding pumping sessions is a game-changer for early postpartum flexibility.
4. Earth Mama Organic Nipple Butter
Best Nipple Care
Lanolin-free, organic nipple balm that does not need to be wiped off before feeding. Made with herbs traditionally used for skin healing including calendula and olive oil.
- USDA Certified Organic
- Safe for baby — no need to remove before nursing
- Non-sticky formula that absorbs well
- Also works on dry skin, cuticles, and lips
Why we recommend it: Many women react to lanolin. This plant-based alternative is gentler and equally effective at preventing and healing cracked nipples.
5. Elvie Stride Hospital-Grade Breast Pump
Best Wearable Breast Pump
Hospital-grade suction in a wearable, in-bra design. No tubes, no wall outlet needed. Lets you pump while walking, cooking, or holding your baby — a radical departure from being tethered to a wall pump.
- Hospital-grade suction (up to 270 mmHg)
- 5 oz capacity per cup
- App-controlled with session tracking
- Quiet motor — usable during calls or while baby sleeps
Why we recommend it: Freedom of movement while pumping directly impacts how consistently mothers pump, which directly impacts supply. Investment pays for itself in reduced supplementation costs.
6. Boppy Original Nursing Pillow
Best Nursing Support Pillow
Wraps around your waist to bring baby to breast height, reducing strain on your neck, shoulders, and arms. The firm-but-giving fill maintains its shape feed after feed.
- Machine-washable slipcover
- Firm support that does not flatten
- Multi-use: tummy time, sitting support for older babies
- Multiple fabric options
Why we recommend it: Proper positioning prevents back pain, improves latch quality, and makes longer feeds sustainable. A nursing pillow is not a luxury — it is ergonomic equipment.
Disclosure: PostpartumSpot.com earns a commission on qualifying purchases through the links above. This does not affect our editorial independence — we only recommend products we have researched and believe in.
Week-by-Week Fourth Trimester Timeline
Understanding the typical trajectory helps you gauge whether your recovery is on track and gives you something to anchor expectations to. Remember: this is a general guide, not a prescription. Your timeline may differ.
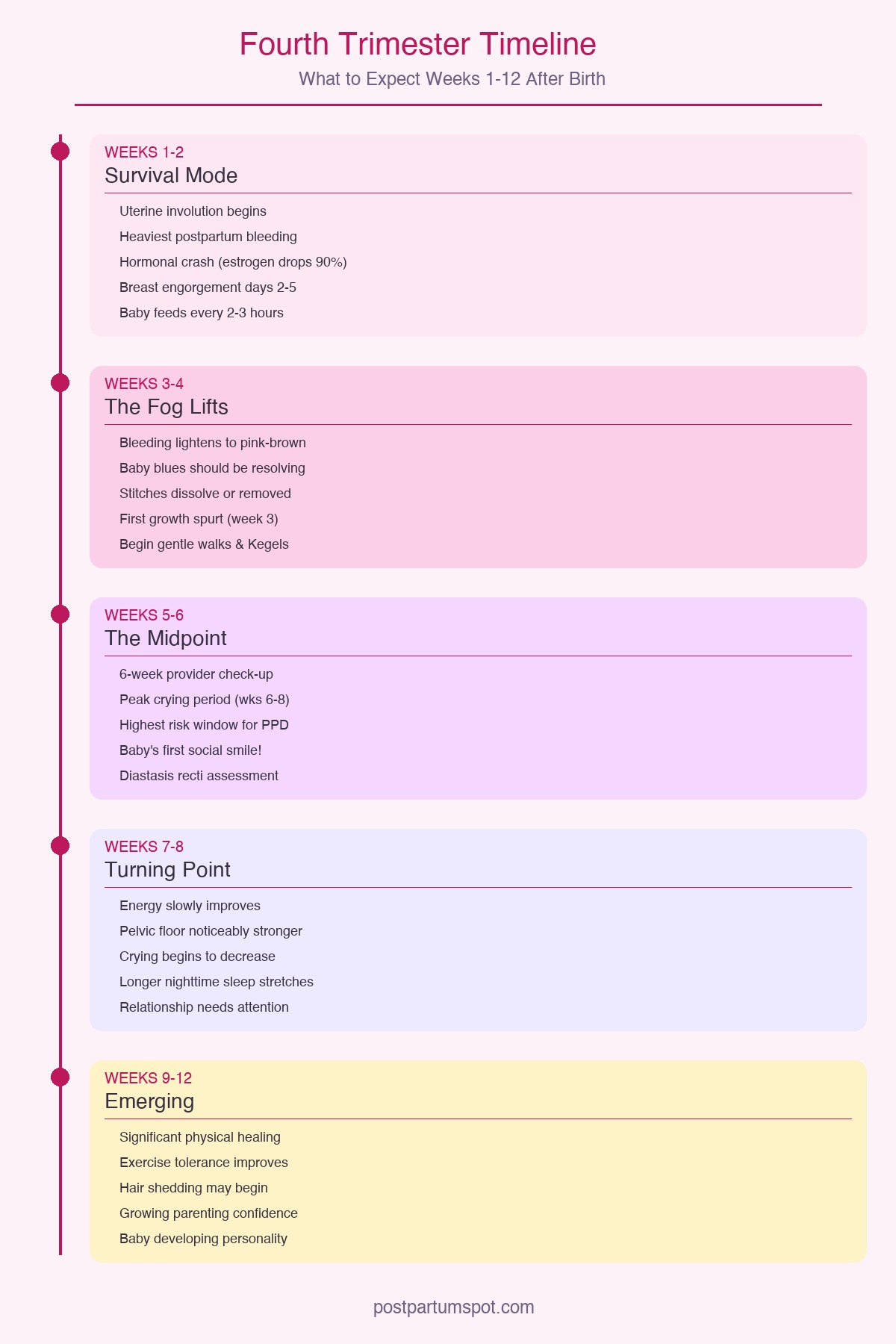
Weeks 1–2: Survival Mode
Your body: Heaviest bleeding, worst afterpains, breast engorgement, significant fatigue. Caesarean mothers are managing surgical pain. Perineal stitches are at their most uncomfortable.
Your mind: Hormonal crash, potential baby blues, hypervigilance, surreal feeling of "is this really my life now?"
Your baby: Sleeps 16–18 hours per day in short bursts. Feeds every 2–3 hours. Loses up to 10% of birth weight (normal) and should regain it by day 10–14.
Priority: Rest, feeding, basic hygiene, pain management. Nothing else matters.
Weeks 3–4: The Fog Lifts Slightly
Your body: Bleeding transitions from red to pinkish-brown. Stitches dissolve or are removed. Engorgement settles as milk supply regulates. Energy may improve marginally.
Your mind: Baby blues should be resolving. If they are not — or if they are intensifying — this is the point to speak with your provider. You may begin to feel small moments of confidence in your parenting ability.
Your baby: More alert wake windows (30–60 minutes). May begin to focus on faces. Feeding patterns may shift with the first growth spurt around week 3.
Priority: Establishing a loose rhythm (not a schedule). Beginning gentle walks and pelvic floor exercises if you had an uncomplicated vaginal birth.
Weeks 5–6: The Midpoint
Your body: Lochia tapers off. Caesarean incision is closing well. Hormonal acne and hair changes may begin. You may have your 6-week provider check-up — advocate for a thorough assessment, not just a rubber stamp.
Your mind: This is statistically the period of highest risk for PPD onset. Fatigue is cumulative and may peak. The initial wave of support from friends and family often fades.
Your baby: Peak crying period (weeks 6–8). Social smiling begins — a milestone that provides enormous emotional fuel for exhausted parents.
Priority: Mental health monitoring. Diastasis recti assessment. Considering gentle exercise beyond walking. Reconnecting with your support network. See our detailed postpartum recovery week-by-week guide for specific milestones.
Weeks 7–8: The Turning Point
Your body: Energy slowly improves. Pelvic floor strength should be noticeably better if you have been doing exercises. Some women resume sexual activity (with care and adequate lubrication — oestrogen levels remain low, especially if breastfeeding).
Your mind: You may start to feel more like yourself. Parenting confidence grows. The relationship with your partner may need deliberate attention after weeks of survival mode.
Your baby: Crying begins to decrease after the week 6–8 peak. Longer wake windows. More interactive. May begin to consolidate one longer stretch of nighttime sleep (3–5 hours).
Priority: Gradually expanding your world. Accepting that "bouncing back" is a harmful myth and that rebuilding takes time.
Weeks 9–12: Emerging
Your body: Significant physical healing has occurred. Exercise tolerance improves. Hair shedding may begin (postpartum telogen effluvium — see our postpartum hair loss guide). Menstruation may return if you are not exclusively breastfeeding.
Your mind: Growing confidence and competence as a parent. Grief for your old life may surface alongside genuine love for your new one. Both can coexist.
Your baby: Developing a personality. Cooing, batting at objects, discovering hands. Sleep may begin to consolidate further. The "fourth trimester" transition from womb to world is completing.
Priority: Looking forward. Considering return-to-work logistics. Maintaining mental health practices. Celebrating how far you have come.
When to Call Your Doctor
The fourth trimester is full of discomforts that are normal. But some symptoms require urgent medical attention. Contact your healthcare provider immediately if you experience:
- Heavy bleeding: Soaking more than one pad per hour, or passing clots larger than a golf ball
- Fever above 38°C (100.4°F): May indicate infection (endometritis, mastitis, wound infection)
- Foul-smelling vaginal discharge: Suggests uterine infection
- Severe headache that does not respond to paracetamol/ibuprofen: Could indicate pre-eclampsia (can develop up to 6 weeks postpartum)
- Visual disturbances, swelling, or upper abdominal pain: Also signs of postpartum pre-eclampsia
- Chest pain, shortness of breath, or leg swelling: Risk of blood clot (postpartum women have a 4–5x increased risk of venous thromboembolism)
- Incision redness, swelling, oozing, or opening: Wound complications
- Thoughts of harming yourself or your baby: This is a medical emergency. Call your provider, go to A&E/the ER, or call the crisis line immediately.
- Inability to eat, sleep (even when given the opportunity), or care for yourself or your baby
Trust your instincts. If something feels wrong, it is worth a call. Healthcare providers would far rather receive a "false alarm" than miss a genuine emergency.
FAQ: Fourth Trimester
How long does the fourth trimester last?
The fourth trimester spans the first 12 weeks (approximately three months) after birth. During this period your body undergoes significant physical healing — uterine involution, tissue repair, hormonal recalibration — while your newborn transitions from womb to world. Some experts argue the adjustment period extends to 6 months, but the 12-week framework is the most widely accepted clinical definition. By the end of the fourth trimester, most acute physical recovery has occurred, though full healing (especially pelvic floor and abdominal wall) can take 6–12 months.
Is it normal to feel disconnected from my baby during the fourth trimester?
Yes. Bonding is not always instant, and the pressure to feel an immediate overwhelming love can make you feel broken when you do not. Hormonal upheaval, exhaustion, birth trauma, pain medication, and the sheer overwhelm of new parenthood can all delay the rush of attachment. Research published in the Archives of Women's Mental Health shows that consistent responsive caregiving — feeding, holding, soothing, being present — builds the bond over weeks, not hours. If feelings of disconnection persist beyond a few weeks, are accompanied by intrusive thoughts, or make it difficult to care for your baby, speak with your healthcare provider. This could indicate PPD, which responds well to treatment.
When should I start exercising after giving birth?
Gentle movement can begin within the first week for uncomplicated vaginal births. This includes pelvic floor exercises (Kegels), gentle stretching, and short walks. After a caesarean, most providers recommend waiting 6–8 weeks before anything beyond light walking. Before returning to structured exercise, get clearance from your midwife or OB-GYN and — ideally — an assessment from a pelvic floor physiotherapist. Check for diastasis recti before doing any abdominal work. See our diastasis recti recovery exercise guide for safe progressions.
What is the difference between baby blues and postpartum depression?
Baby blues affect up to 80% of new mothers, begin around days 3–5, and resolve within two weeks. Symptoms include tearfulness, mood swings, irritability, and feeling overwhelmed. They are caused by the dramatic hormonal drop after delivery and do not require treatment.
Postpartum depression is a clinical condition affecting approximately 1 in 7 new mothers. It lasts longer than two weeks, is more severe, and interferes with your ability to function. Symptoms include persistent sadness, loss of interest, difficulty bonding with your baby, changes in appetite or sleep beyond what baby-related disruption causes, feelings of worthlessness, and sometimes thoughts of self-harm. PPD requires professional treatment — typically therapy, medication, or both. If you are unsure which you are experiencing, our postpartum anxiety vs. depression guide can help you identify your symptoms.
Can partners experience the fourth trimester too?
Absolutely. Partners undergo their own version of the fourth trimester. Studies published in Hormones and Behavior show that new fathers experience measurable hormonal changes: testosterone drops by 10–30%, while oxytocin and prolactin levels rise. These shifts support caregiving behaviour but also contribute to mood changes.
Approximately 10% of new fathers experience paternal postnatal depression — a figure that doubles when the birthing partner has PPD. Partners also face sleep deprivation, identity shifts, relationship strain, and often pressure to be "the strong one" while receiving little support themselves. Partners benefit from their own support networks, honest communication with the birthing parent, and should not hesitate to seek professional help if they are struggling.
How can I tell if my bleeding is normal or a sign of something serious?
Postpartum bleeding (lochia) is normal and can last 4–6 weeks. It follows a predictable pattern: bright red and heavy in the first few days, transitioning to pink-brown by week 2, and then to yellowish-white before stopping. Warning signs that require immediate medical attention include soaking more than one pad per hour, passing clots larger than a golf ball, a sudden return of bright red bleeding after it had already lightened, foul-smelling discharge, or bleeding accompanied by fever or dizziness. When in doubt, call your provider — they would rather hear from you unnecessarily than miss something serious.
Sources
-
American College of Obstetricians and Gynecologists (ACOG). "Optimizing Postpartum Care." ACOG Committee Opinion No. 736, May 2018 (reaffirmed 2025). acog.org
-
Hoekzema, E. et al. "Pregnancy leads to long-lasting changes in human brain structure." Nature Neuroscience, vol. 20, 2017, pp. 287–296. Landmark neuroimaging study demonstrating structural brain changes in new mothers.
-
Barr, R.G. "The Period of PURPLE Crying." National Center on Shaken Baby Syndrome, 2024. Evidence-based framework for understanding normal infant crying patterns.
-
O'Hara, M.W. and McCabe, J.E. "Postpartum Depression: Current Status and Future Directions." Annual Review of Clinical Psychology, vol. 9, 2013, pp. 379–407.
-
Woodley, S.J. et al. "Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women." Cochrane Database of Systematic Reviews, 2020. Systematic review supporting pelvic floor exercise in postpartum recovery.
-
Sperstad, J.B. et al. "Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain." British Journal of Sports Medicine, vol. 50, no. 17, 2016, pp. 1092–1096.
-
Saxbe, D. et al. "Fathers' decline in testosterone and synchrony with partner testosterone during pregnancy predicts greater postpartum relationship investment." Hormones and Behavior, vol. 90, 2017, pp. 66–75.
About the Author
Dr. Nina Chen is a board-certified OB-GYN and postpartum specialist with over 15 years of experience in maternal health. She completed her residency at Johns Hopkins Hospital and fellowship in maternal-fetal medicine at UCSF. Dr. Chen is a clinical advisor to the Postpartum Support International (PSI) helpline, has published extensively in peer-reviewed journals on postpartum recovery and mental health, and is a passionate advocate for extending the standard of postpartum care beyond the traditional six-week check-up. She currently practises in San Francisco, where she runs a specialised fourth trimester clinic.
Have questions about your fourth trimester recovery? Reach out to our editorial team at editorial@postpartumspot.com.
Visual Guide Gallery