TMJ Guide
Diastasis Recti: How to Know If You Have It and Fix It
How long does it take to heal diastasis recti?
By Expert Team · Published 2026-03-10 · Updated 2026-03-10
Diastasis recti is a separation of the left and right sides of the rectus abdominis muscle along the linea alba, most commonly caused by pregnancy. It affects up to 60% of postpartum women and can cause a visible belly "pooch," lower back pain, and pelvic floor dysfunction. The good news: targeted exercises and lifestyle changes can close the gap without surgery in most cases.
By Dr. Emily Chen, Perinatal Mental Health Specialist Last updated: March 2026
Table of Contents
- What Is Diastasis Recti?
- What Causes Diastasis Recti?
- Signs and Symptoms
- The Self-Check Finger Test
- Grading the Severity of Your Separation
- Exercises You Must Avoid
- 8 Safe Healing Exercises for Diastasis Recti
- Building a Weekly Exercise Plan
- Supportive Products That Help Recovery
- When to See a Physiotherapist or Surgeon
- Diastasis Recti and Your Pelvic Floor
- FAQ
- Sources
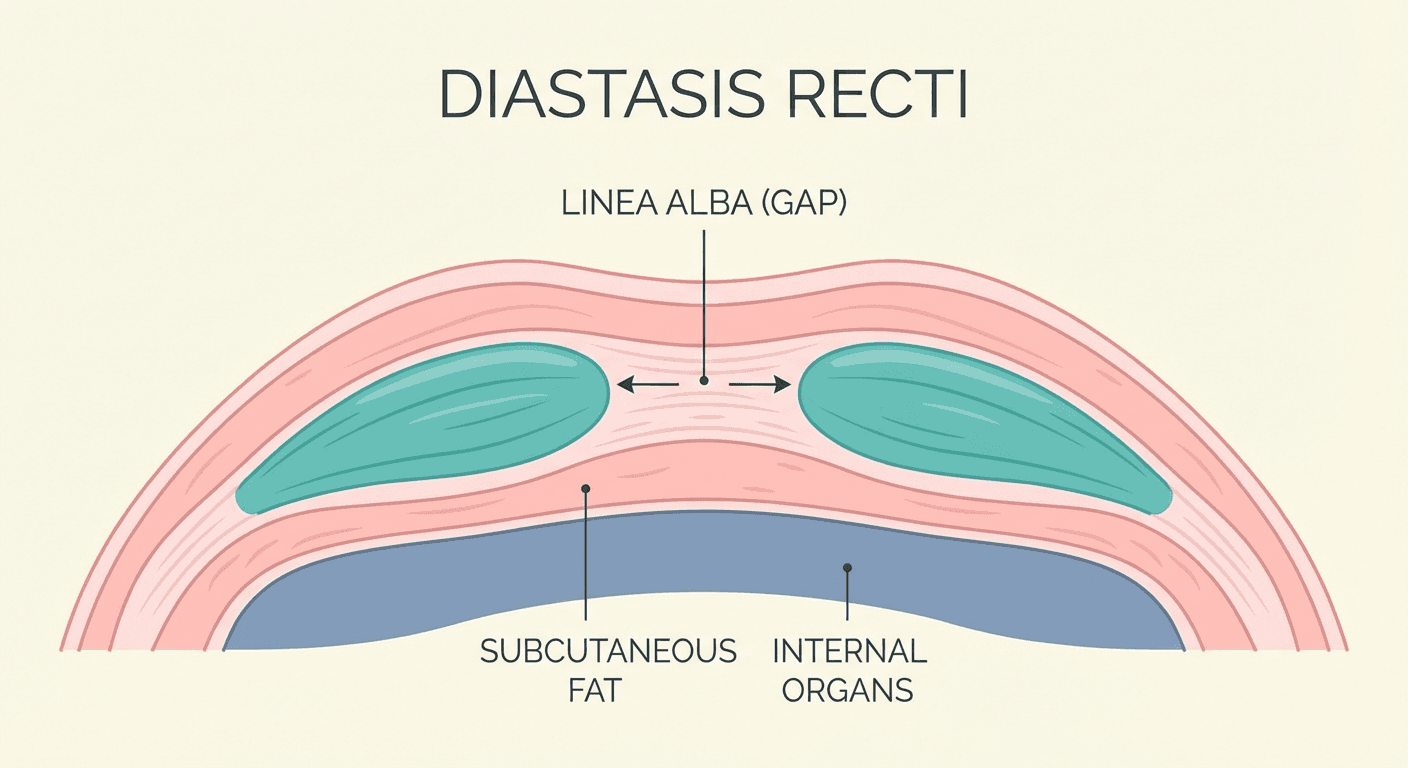
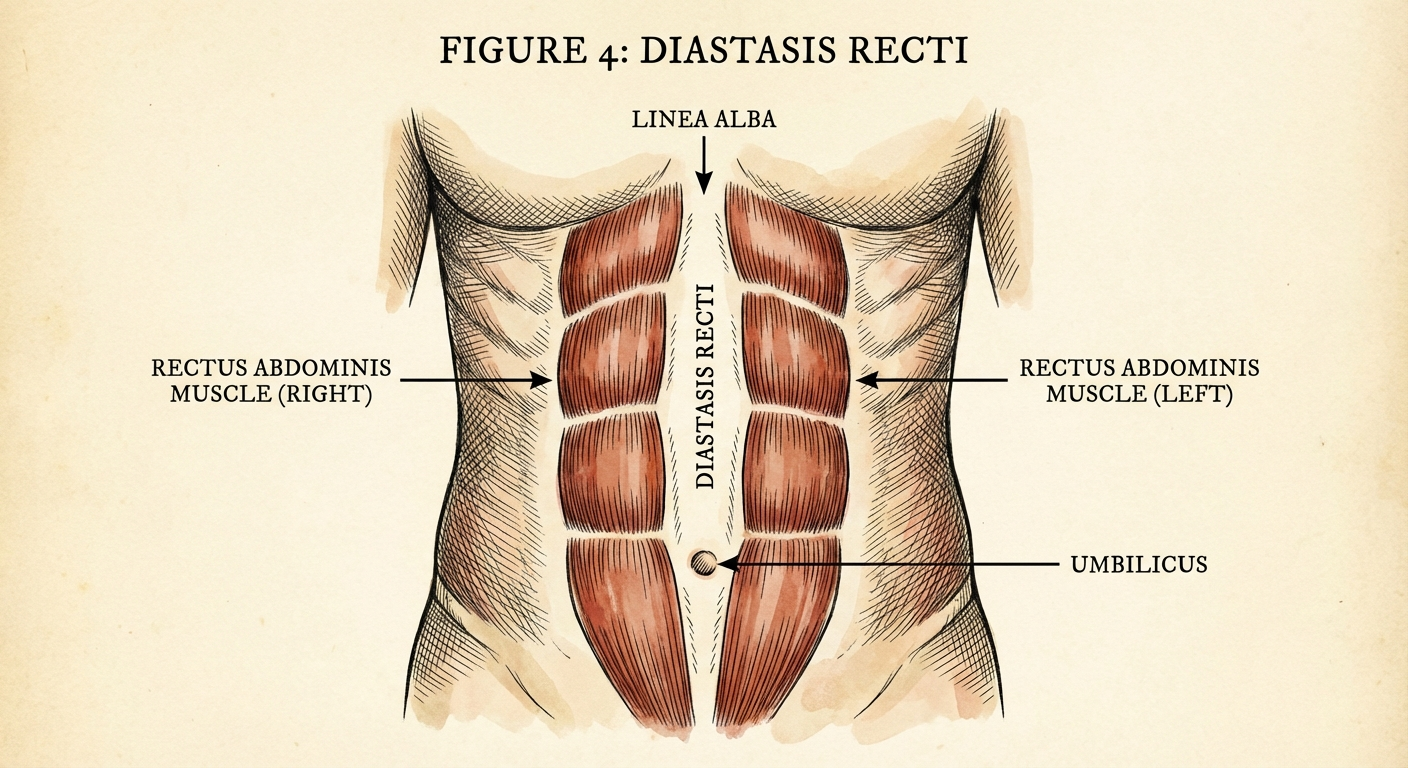
What Is Diastasis Recti?
Diastasis recti — sometimes called abdominal separation or "diastasis recti abdominis" (DRA) — occurs when the two parallel bands of the rectus abdominis muscle separate along the midline connective tissue known as the linea alba. This connective tissue stretches and thins, creating a gap that can range from one to several finger-widths wide.
During pregnancy, rising levels of the hormone relaxin soften connective tissue throughout the body to prepare for childbirth. Combined with the mechanical pressure of a growing uterus, the linea alba stretches to accommodate the baby. For many women, this tissue rebounds naturally in the weeks following delivery. However, for a significant percentage — studies suggest between 33% and 60% of postpartum women — the gap persists beyond the first eight weeks.
Diastasis recti is not limited to postpartum women. It can also affect men, non-pregnant women, and even newborn infants. However, the condition is overwhelmingly associated with pregnancy and the postpartum period, which is the focus of this guide.
If you are in the early stages of postpartum recovery, our comprehensive postpartum recovery guide covers the broader timeline of physical healing and when it is safe to begin targeted exercises.
What Causes Diastasis Recti?
Understanding the root causes helps you take preventive steps during pregnancy and make better decisions about recovery afterward.
Primary Causes
- Pregnancy: The expanding uterus places sustained outward pressure on the abdominal wall over the course of nine months. This is the single most common cause.
- Hormonal changes: Relaxin and progesterone loosen connective tissues, making the linea alba more susceptible to stretching.
- Multiple pregnancies: Each subsequent pregnancy increases the risk because the connective tissue may not have fully recovered between pregnancies.
- Carrying multiples: Twin or higher-order pregnancies place greater mechanical load on the abdominal wall.
Contributing Risk Factors
- Age over 35 at delivery: Connective tissue elasticity naturally declines with age.
- High birth-weight baby: Larger babies create more intra-abdominal pressure.
- Poor core engagement habits: Chronic bearing down, breath-holding during exertion, or improper lifting technique can worsen the separation.
- Excessive abdominal exercises during late pregnancy: Performing traditional crunches or sit-ups in the second and third trimesters can accelerate the separation.
- Obesity or rapid weight gain: Additional adipose tissue around the midsection increases strain on the linea alba.
- Genetics: Some women have naturally thinner or less resilient connective tissue.
Signs and Symptoms
Diastasis recti does not always produce dramatic symptoms, which is why so many women live with it unknowingly. Common signs include:
- A visible ridge or bulge running down the center of the abdomen, especially when you contract your abs (such as when sitting up from a lying position)
- A "doming" or "coning" appearance of the belly during exertion
- Persistent lower back pain that does not improve with rest
- A feeling of weakness in the core, as if your trunk cannot support you properly
- Pelvic floor issues such as urinary incontinence or pelvic organ prolapse
- Bloating or a "pooch" that remains despite returning to pre-pregnancy weight
- Difficulty lifting heavy objects or performing everyday tasks that require core stability
- Poor posture and a tendency to lean backward when standing
It is worth noting that having a visible belly after pregnancy is completely normal and does not automatically indicate diastasis recti. The self-check test described below will help you determine whether a true muscular separation is present.
The Self-Check Finger Test
The finger-width test is a simple, at-home method to screen for diastasis recti. It is not a replacement for a professional assessment, but it gives you a reliable starting point.
How to Perform the Test
- Lie on your back on a firm surface with your knees bent and feet flat on the floor, hip-width apart.
- Place one hand behind your head for support.
- Position two or three fingers of your other hand horizontally across your midline, just above your belly button, fingertips pointing toward your toes.
- Slowly lift your head and shoulders off the floor as if beginning a crunch. You do not need to lift far — just enough to engage the rectus abdominis.
- Feel for a gap between the two muscle walls. Your fingers will sink into the space if a separation exists.
- Measure the width of the gap in finger-widths. Also note the depth — can your fingers sink in deeply, or is there firm tension beneath them?
- Repeat the test at three points: two inches above the navel, directly at the navel, and two inches below the navel. The separation can vary at each level.
What Your Results Mean
- 1 finger-width or less: Normal. No clinical diastasis recti.
- 1.5 to 2 finger-widths: Mild diastasis recti. Likely to respond well to targeted exercises.
- 2 to 3 finger-widths: Moderate diastasis recti. Targeted exercise is still the first-line treatment, but consider a professional assessment.
- More than 3 finger-widths: Significant separation. Seek evaluation from a pelvic floor physiotherapist or a healthcare provider experienced in postpartum recovery.
The depth and tension of the gap matter as much as the width. A two-finger-width gap with firm, springy tissue beneath it may be more functional than a one-finger-width gap where your fingers sink deeply with no resistance.
Grading the Severity of Your Separation
Healthcare professionals generally classify diastasis recti into mild, moderate, and severe categories based on the inter-recti distance (IRD) measured either by calipers, ultrasound, or the finger-width method described above.
| Severity | Gap Width | Characteristics | Typical Approach |
|---|---|---|---|
| Mild | 1.5–2 cm (about 1–2 fingers) | Slight visible bulge, minimal functional impairment | Home exercise program |
| Moderate | 2–3 cm (about 2–3 fingers) | Noticeable doming with exertion, possible back pain | Guided exercise + possible physio |
| Severe | >3 cm (more than 3 fingers) | Significant bulge, functional limitations, possible hernia | Physiotherapy evaluation, possible surgical consult |
It is important to understand that the raw number does not tell the whole story. A physiotherapist will also assess the quality of the connective tissue, your overall core function, and whether you have accompanying pelvic floor issues. Many women with a two-finger-width gap function perfectly well, while others with a narrower gap experience significant symptoms.
Exercises You Must Avoid
Before we cover what to do, it is critical to understand what not to do. Certain movements increase intra-abdominal pressure in a way that pushes the abdominal wall outward, worsening the separation.
Exercises to Avoid Until the Gap Closes
- Traditional crunches and sit-ups: These create intense forward pressure on the linea alba.
- Full planks and push-ups (unsupported): These load the anterior abdominal wall heavily before it is ready.
- Double leg lifts: Lifting both legs simultaneously while lying on your back dramatically increases intra-abdominal pressure.
- Twisting movements under load: Russian twists, bicycle crunches, and similar exercises stress the obliques in a way that can pull the rectus abdominis further apart.
- Heavy overhead pressing: Pressing heavy weights overhead without adequate core bracing can worsen the gap.
- Burpees and box jumps: High-impact movements that challenge core stability before it has been rebuilt.
Daily Movements to Modify
- Getting out of bed: Roll to your side and push up with your arms rather than sitting straight up.
- Lifting your baby or toddler: Exhale and gently engage your deep core before lifting. Avoid holding your breath.
- Coughing or sneezing: Support your abdomen with your hands or a pillow during strong coughs.
8 Safe Healing Exercises for Diastasis Recti
The following exercises are ordered from least to most challenging. Start with exercises 1 through 3 in your first two weeks, then progressively add the remaining exercises as your strength and control improve. Each exercise focuses on training the transverse abdominis (the deepest core muscle), improving coordination between the core and pelvic floor, and restoring functional tension to the linea alba.
Always listen to your body. If you see doming or coning along the midline during any exercise, stop and regress to an easier variation.
1. Diaphragmatic Breathing (Connection Breath)
Why it helps: This foundational exercise teaches you to coordinate your diaphragm and pelvic floor, creating balanced intra-abdominal pressure rather than the outward-pushing pressure that worsens diastasis recti.
How to do it:
- Lie on your back with knees bent, feet flat on the floor.
- Place one hand on your chest and the other on your lower belly.
- Inhale slowly through your nose for 4 counts, directing the breath into your lower ribcage and belly. Your lower hand should rise gently.
- Exhale slowly through pursed lips for 6 counts. As you exhale, feel your pelvic floor gently lift and your belly draw inward naturally — do not force it.
- Repeat for 10 breaths, 3 times per day.
Progression: Once comfortable lying down, practice while seated, then standing, and finally during functional movements.
2. Heel Slides
Why it helps: Heel slides challenge your deep core to stabilize the pelvis while one leg moves, building the foundation for more complex movements.
How to do it:
- Lie on your back with knees bent, feet flat.
- Exhale and gently engage your core (think about drawing your hip bones together).
- Slowly slide one heel along the floor until your leg is fully extended.
- Inhale as you slide the heel back to the starting position.
- Alternate sides. Perform 10 repetitions per side, 2–3 sets.
Key cue: Your pelvis and lower back should remain completely still. If your back arches off the floor, the exercise is too advanced — reduce the range of motion.
3. Dead Bug (Modified)
Why it helps: The dead bug trains anti-extension — your core's ability to resist arching — which directly supports the linea alba.
How to do it:
- Lie on your back. Lift your legs to a tabletop position (hips and knees both at 90 degrees). Arms extended toward the ceiling.
- Exhale and slowly lower your right arm overhead and your left leg toward the floor simultaneously.
- Only go as far as you can while keeping your lower back pressed firmly into the floor.
- Inhale and return to the starting position. Alternate sides.
- Perform 8 repetitions per side, 2–3 sets.
Regression: If controlling both limbs is too much, start by lowering only one leg at a time with arms stationary.
4. Bird-Dog
Why it helps: This exercise challenges core stability in a hands-and-knees position, which reduces gravitational load on the abdominal wall while building coordination.
How to do it:
- Start on all fours with wrists under shoulders and knees under hips. Maintain a neutral spine.
- Exhale and simultaneously extend your right arm forward and your left leg backward until both are parallel to the floor.
- Hold for 2–3 seconds, focusing on keeping your hips level and your core engaged.
- Inhale and return to the starting position. Alternate sides.
- Perform 8 repetitions per side, 2–3 sets.
Key cue: Imagine you are balancing a glass of water on your lower back. If your hips rock side to side, reduce the range of motion or extend only the arm or only the leg until you build more stability.
5. Modified Plank (Incline or Knee Plank)
Why it helps: Planks train the entire core as a unit, but a full plank is too demanding early in recovery. An incline or knee variation reduces the load while still building endurance.
How to do it:
- Place your forearms on an elevated surface such as a bench, couch, or countertop. The higher the surface, the easier the exercise.
- Step your feet back so your body forms a straight line from head to heels (or head to knees if performing a knee plank on the floor).
- Exhale and engage your core. Hold the position for 15–30 seconds.
- Build up to 3 sets of 30–45 seconds.
Progression: Gradually lower the surface height over weeks until you can perform a forearm plank on the floor without doming.
6. Pallof Press
Why it helps: The Pallof press is an anti-rotation exercise that strengthens the obliques and transverse abdominis without creating the shearing forces that worsen diastasis recti.
How to do it:
- Attach a resistance band to a door handle or sturdy anchor point at chest height. Stand perpendicular to the anchor.
- Hold the band at your chest with both hands. Step far enough away to create moderate tension.
- Exhale and press the band straight out in front of you, extending your arms fully. The band will try to rotate you toward the anchor — resist this.
- Hold for 2–3 seconds, then bring the band back to your chest.
- Perform 10 repetitions per side, 2–3 sets.
Key cue: Your hips and shoulders should face straight ahead throughout the entire movement. If you feel yourself twisting, reduce the resistance.
7. Clamshells
Why it helps: Clamshells strengthen the gluteus medius, which plays a critical role in pelvic stability. Weak glutes force the core to compensate, which can aggravate diastasis recti.
How to do it:
- Lie on your side with knees bent at 45 degrees, hips stacked, and head resting on your lower arm.
- Keep your feet together and exhale as you open your top knee toward the ceiling, like a clamshell opening.
- Raise the knee as high as you can without your pelvis rolling backward.
- Slowly lower the knee back down. Perform 15 repetitions per side, 2–3 sets.
Progression: Add a resistance band just above your knees for added challenge.
8. Glute Bridge
Why it helps: The glute bridge reinforces the posterior chain (glutes and hamstrings) while training the core to stabilize in a hip-extension pattern — a movement you perform constantly in daily life.
How to do it:
- Lie on your back with knees bent, feet flat on the floor, hip-width apart.
- Exhale and squeeze your glutes to lift your hips toward the ceiling until your body forms a straight line from shoulders to knees.
- Hold for 2–3 seconds at the top. Avoid overarching your lower back.
- Slowly lower back down. Perform 12 repetitions, 3 sets.
Progression: Try single-leg glute bridges once you can comfortably perform 15 double-leg repetitions with good form.
Building a Weekly Exercise Plan
Consistency matters more than intensity. Here is a sample four-week progression:
Weeks 1–2: Diaphragmatic breathing (daily), heel slides (3x/week), modified dead bug (3x/week). Total session time: 10–15 minutes.
Weeks 3–4: Add bird-dog and clamshells to your routine. Continue breathing work daily. Total session time: 15–20 minutes.
Weeks 5–6: Add modified plank and glute bridge. Begin reducing rest times between sets. Total session time: 20–25 minutes.
Weeks 7–8: Add Pallof press. Retest your gap width using the finger test. Total session time: 25–30 minutes.
After eight weeks, many women see measurable improvement. If your gap has narrowed and your core feels more functional, continue progressing the exercises by adding resistance, duration, or complexity. If you have not seen meaningful change, it is time to consult a pelvic floor physiotherapist.
For exercises that strengthen the pelvic floor alongside your diastasis recti recovery, read our guide on pelvic floor exercises after birth.
Supportive Products That Help Recovery
While exercises are the foundation of healing, certain products can support your recovery — especially in the early postpartum weeks.
Postpartum Belly Wraps and Binders
A well-fitted postpartum belly wrap provides gentle compression that supports the abdominal wall and can improve proprioceptive awareness of your core. They are most useful in the first 8–12 weeks postpartum. We have a detailed comparison of the best options in our best postpartum belly wrap guide.
Browse top-rated postpartum belly wraps on Amazon
Resistance Bands for Home Exercise
A set of looped resistance bands is essential for exercises like the Pallof press and banded clamshells. Look for a set with multiple resistance levels so you can progress over time.
Browse resistance band sets on Amazon
Supportive Exercise Mat
A thick, cushioned exercise mat protects your spine during floor work and makes your daily exercise sessions more comfortable — which means you are more likely to stick with the program.
Browse thick exercise mats on Amazon
When to See a Physiotherapist or Surgeon
Most cases of diastasis recti respond well to conservative treatment through targeted exercise. However, there are situations where professional guidance is essential.
See a Pelvic Floor Physiotherapist If:
- Your gap has not improved after 8–12 weeks of consistent, targeted exercise.
- You experience pelvic floor symptoms alongside your diastasis recti, such as urinary leakage, pelvic pressure, or pain during intercourse.
- You are unsure whether you are performing exercises correctly or experiencing doming during movements.
- Your separation is moderate to severe (more than 2.5 finger-widths).
- You have back pain that interferes with daily activities.
A pelvic floor physiotherapist can perform an ultrasound assessment to measure the gap precisely, evaluate the quality of your connective tissue, assess your pelvic floor function, and design a personalized rehabilitation program.
Consider a Surgical Consultation If:
- Conservative treatment has been followed diligently for 6–12 months with minimal improvement.
- You have a concurrent hernia (a true bulge of tissue through the abdominal wall).
- The separation is severe and causes significant functional limitations.
- You have completed your family and do not plan future pregnancies (as pregnancy would likely reopen the repair).
The most common surgical procedure is abdominoplasty with rectus plication, where the surgeon sutures the rectus abdominis muscles back together. Some surgeons now perform minimally invasive laparoscopic repair. Surgery is generally considered a last resort after conservative treatment has been fully explored.
Diastasis Recti and Your Pelvic Floor
Diastasis recti and pelvic floor dysfunction are closely linked. The abdominal wall and pelvic floor work as a coordinated pressure management system. When the abdominal wall cannot manage intra-abdominal pressure effectively (as in diastasis recti), the pelvic floor absorbs the excess load, which can lead to:
- Stress urinary incontinence (leaking when coughing, sneezing, or jumping)
- Pelvic organ prolapse (a feeling of heaviness or bulging in the vaginal area)
- Pelvic pain during exercise or intercourse
This is why the diaphragmatic breathing exercise listed first in the program above is so important — it teaches the diaphragm, core, and pelvic floor to work together as an integrated unit. When you rehabilitate diastasis recti, you should always address pelvic floor function simultaneously.
Our detailed guide on pelvic floor exercises after birth pairs well with the diastasis recti program outlined in this article.
FAQ
How long does it take to heal diastasis recti? With consistent targeted exercise performed 3–5 times per week, most women see measurable improvement within 6–12 weeks. Mild cases may close within a month, while moderate to severe separations can take 6 months or longer. Factors such as the severity of the separation, consistency of exercise, breastfeeding status, and overall health influence the timeline.
Can diastasis recti heal on its own without exercise? Some degree of natural recovery occurs in the first eight weeks postpartum as hormone levels normalize and the uterus returns to its pre-pregnancy size. However, research shows that spontaneous full closure beyond eight weeks is uncommon. Targeted exercise significantly improves outcomes compared to watchful waiting alone.
Is diastasis recti the same as a hernia? No. Diastasis recti is a stretching of the connective tissue (linea alba) between the rectus abdominis muscles. A hernia involves a true defect or tear in the abdominal wall through which tissue or organs can protrude. However, the two conditions can coexist, so a professional assessment is important if you notice a painful or hard bulge.
Will wearing a belly wrap fix diastasis recti? A belly wrap alone will not close the gap. However, a well-fitted wrap can provide external support, improve posture awareness, and reduce discomfort in the early postpartum weeks while you begin your exercise program. Think of it as a supportive tool, not a treatment. See our best postpartum belly wrap guide for recommendations.
Can I do diastasis recti exercises while breastfeeding? Yes. There is no conflict between breastfeeding and performing diastasis recti rehabilitation exercises. In fact, the relaxin hormone associated with breastfeeding may keep connective tissue slightly more pliable, but this does not prevent healing. Stay well hydrated, maintain adequate caloric intake, and avoid aggressive caloric restriction while breastfeeding.
When can I return to running or high-impact exercise? Most pelvic floor physiotherapists recommend waiting until at least 12 weeks postpartum before returning to running, and only after your core and pelvic floor can manage impact without symptoms such as leaking, heaviness, or visible doming. If you have diastasis recti, work through a progressive strengthening program first and consider a professional clearance before resuming high-impact activity.
Can men get diastasis recti? Yes. While less common, men can develop diastasis recti due to obesity, improper exercise technique (especially heavy lifting with poor core bracing), or certain medical conditions. The same principles of rehabilitation apply.
Sources
-
Sperstad, J.B., Tennfjord, M.K., Hilde, G., Ellström-Engh, M., & Bø, K. (2016). Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain. British Journal of Sports Medicine, 50(17), 1092–1096. https://bjsm.bmj.com/content/50/17/1092
-
Mota, P., Pascoal, A.G., Carita, A.I., & Bø, K. (2015). Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Manual Therapy, 20(1), 200–205. https://pubmed.ncbi.nlm.nih.gov/25282439/
-
Benjamin, D.R., van de Water, A.T.M., & Peiris, C.L. (2014). Effects of exercise on diastasis of the rectus abdominis muscle in the antenatal and postnatal periods: a systematic review. Physiotherapy, 100(1), 1–8. https://pubmed.ncbi.nlm.nih.gov/24268942/
-
Gluppe, S., Engh, M.E., & Bø, K. (2021). Immediate effect of abdominal and pelvic floor muscle exercises on interrecti distance in women with diastasis recti abdominis who were parous. Physical Therapy, 101(8), pzab108. https://pubmed.ncbi.nlm.nih.gov/33989397/
Visual Guide Gallery






Walking Pad vs Treadmill
30-second comparison